- Get link
- X
- Other Apps
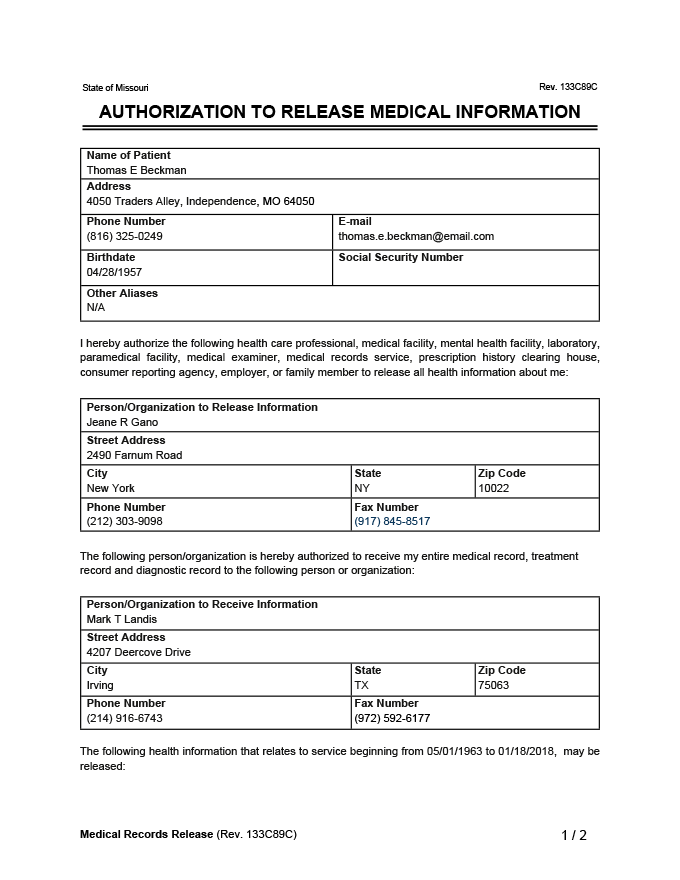
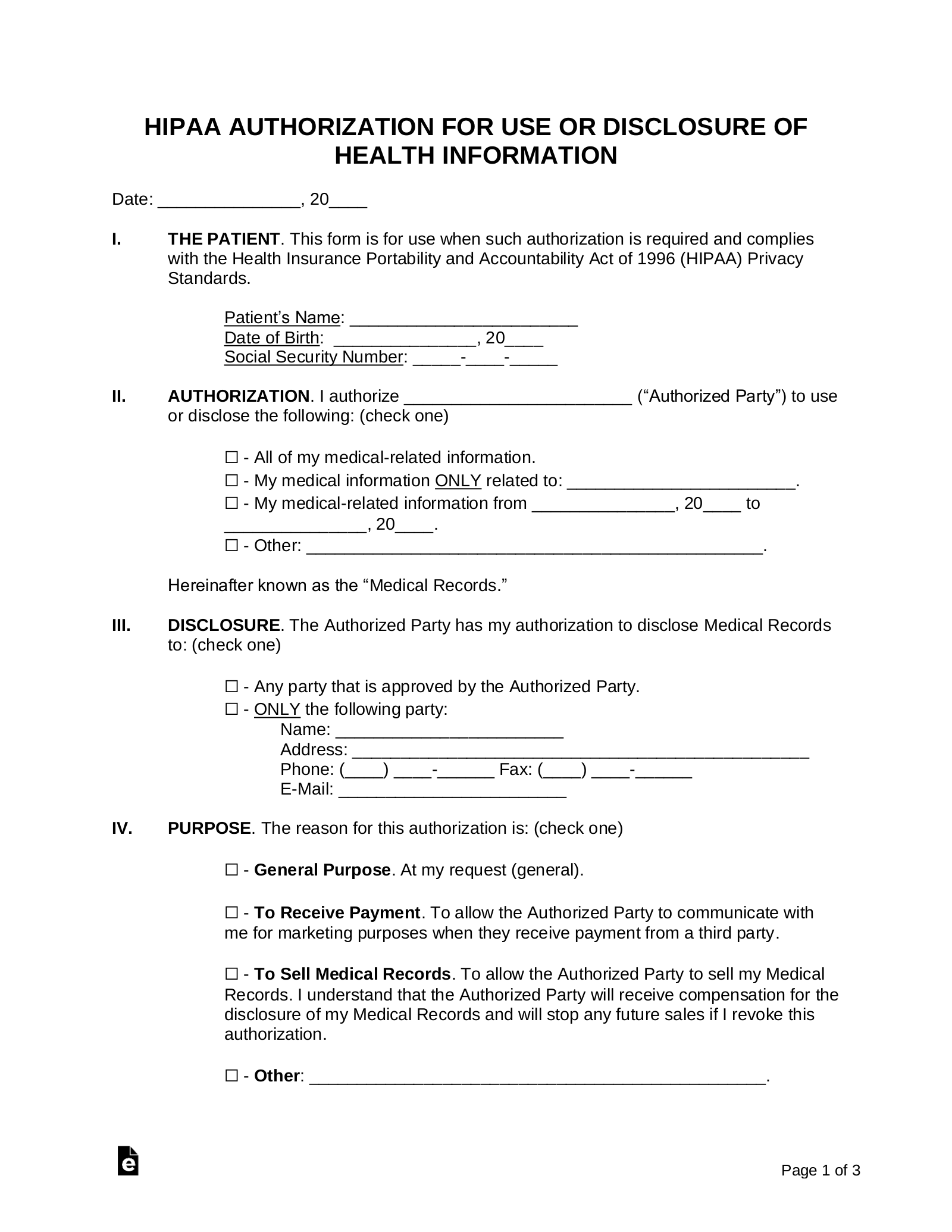
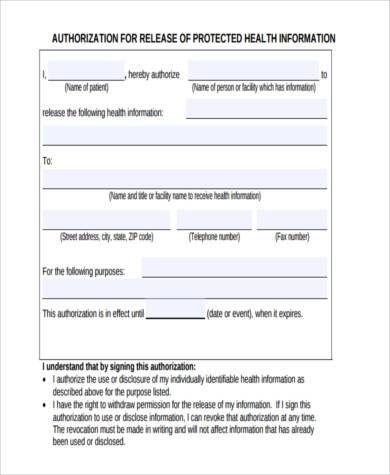
This authorization covers materials considered hospital records reasonably capable of being reduced to printed form. Check the applicable box to indicate to whom you authorize the release of your medical info.
 Medical Records Release Form Generic Request Template Pdf
Medical Records Release Form Generic Request Template Pdf
This form is free to download.

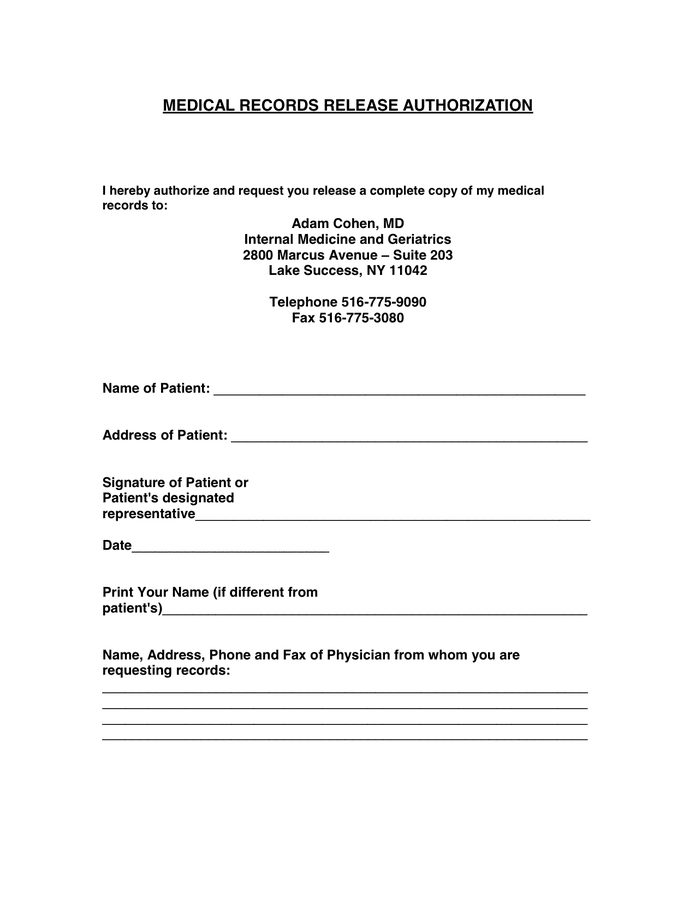
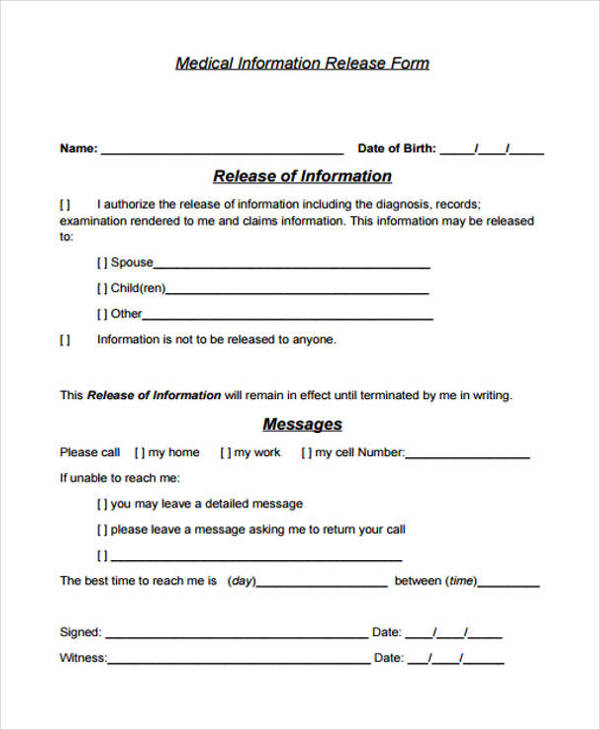
Medical release authorization form. Sample Authorization Form to Release Medical Record 02. This form template authorizes your healthcare provider to release your private medical records to the parties you specify. If not the patient name of person signing form.
Free Blood Pressure Chart and Log Sheets Word PDF. THIS AUTHORIZATION WILL NOT BE ACCEPTED UNLESS ALL ITEMS ARE COMPLETED. A Release Authorization Form is used to obtain the following.
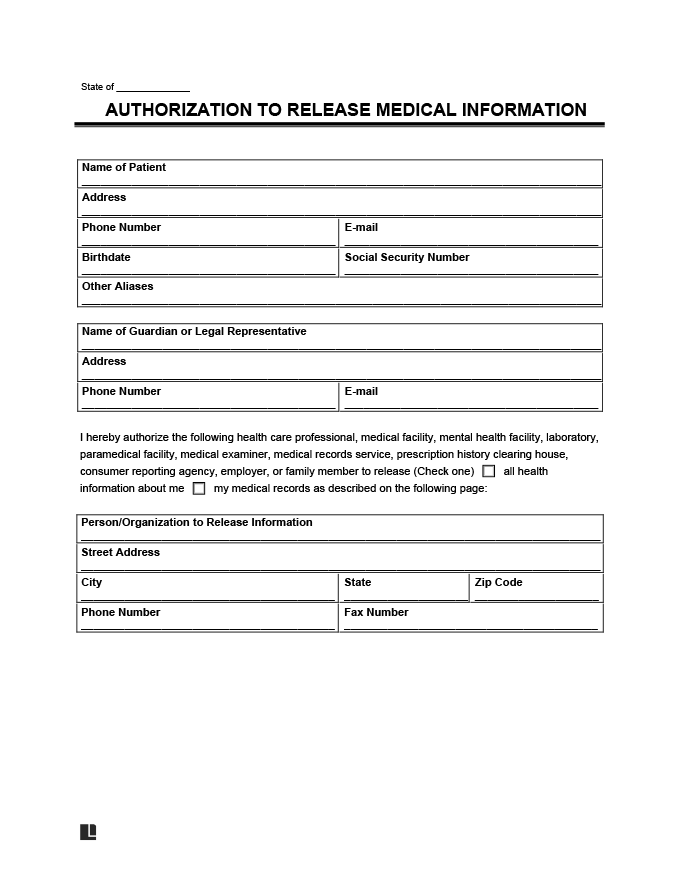
AUTHORIZATION FOR RELEASE OF MEDICAL INFORMATION PATIENT INFORMATION First Name Last Name MaidenOther Names Date of Birth - Address Phone Number City State ZIP Code RELEASE INFORMATION FROM I authorize Northwestern Memorial HealthCare NMHC and its clinical affiliates to release information from check all that apply. The form can either be limited in scope or can be as broad as granting access to the third parties to anything in your medical records. 51 rows The medical record information release HIPAA also known as the Health Insurance.
This document authorizes release of information entered into my medical record prior to or within 12 months after the date of my signature PLEASE RETURN THIS FORM IMMEDIATELY TO HEALTH INFORMATION MANAGEMENT 717-531-5068. Authority to sign on behalf of patient. Step 1 Download in Adobe PDF.
Medical records release forms are forms that give a set of permissions to people in certain situations to allow a clinic hospital or medical professional to release medical records. Medical data and records This requires the use of a Medical Authorization Form which will indicate the particular data that the physician or the healthcare providers will need from their patient. Under HIPAA regulations its referred to as an authorization.
All items on this form have been completed and my questions about this form have been answered. Step 2 Enter your name and your date of birth in the first two fields. The Generic Authorization Medical Release Form is a template of authorization for the release of patient information.
You may also like. At request of individual Other. 1062020 Authorization to release healthcare information.
5162018 Sample Authorization Form to Release Medical Record 01. AUTHORIZATION FOR RELEASE OF MEDICAL RECORDS TO REQUEST RELEASE OF MEDICAL INFORMATION PLEASE COMPLETE AND SIGN THIS FORM I _____hereby voluntarily authorize the disclosure of information from my health record. This form includes the necessary information of the patient the legal statement of the authorization the concrete content that will be released and the signatures of the related person.
Date or event on which this authorization will expire. Advance Directive Medical Power of Attorney and Living Will Do Not Resuscitate Order DNR Forms. HIPAA Medical Release Authorization Form.
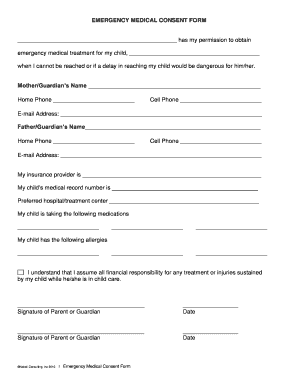
Also this form cannot be used for disclosure of psychotherapy notes. Name of Patient Patient Information. 12262016 A medical release form is a document that gives healthcare professionals permission to share patient medical information with other parties.
What is a Medical Authorization Form. Medical Records Release Authorization Form. If you agree to the request of sharing your medical history with someone who has requested for it you can use this form to request a doctor to release the data as soon as heshe reads the content of this form.
Reason for release of information. Health information shared you need to use Form Florida AHCA FC4200005 Universal Patient Authorization Form For Limited Disclosure of Health Information instead of this form. A medical authorization form is a form from the patient to a third party permitting them to access your protected medical records.
Methodist Le Bonheur Healthcare and its affiliates are hereby released from all legal liability that may arise from the release of the information requested. In order to pass on your medical information you must authorize it by utilizing a medical records release form.


 23 Printable Medical Release Form Templates Fillable Samples In Pdf Word To Download Pdffiller
23 Printable Medical Release Form Templates Fillable Samples In Pdf Word To Download Pdffiller
 Medical Records Release Authorization In Word And Pdf Formats
Medical Records Release Authorization In Word And Pdf Formats
 Free Medical Records Release Authorization Form Hipaa Word Pdf Eforms
Free Medical Records Release Authorization Form Hipaa Word Pdf Eforms
 Free 9 Sample Authorization Release Forms In Pdf Ms Word
Free 9 Sample Authorization Release Forms In Pdf Ms Word
 Free 23 Patient Release Forms In Pdf Ms Word
Free 23 Patient Release Forms In Pdf Ms Word
 Medical Records Release Form Generic Request Template Pdf
Medical Records Release Form Generic Request Template Pdf
 10 Printable Medical Authorization Forms Pdf Doc Free Premium Templates
10 Printable Medical Authorization Forms Pdf Doc Free Premium Templates
 Medical And Financial Records Release Form Fill Online Printable Fillable Blank Pdffiller
Medical And Financial Records Release Form Fill Online Printable Fillable Blank Pdffiller

Medical Release Form
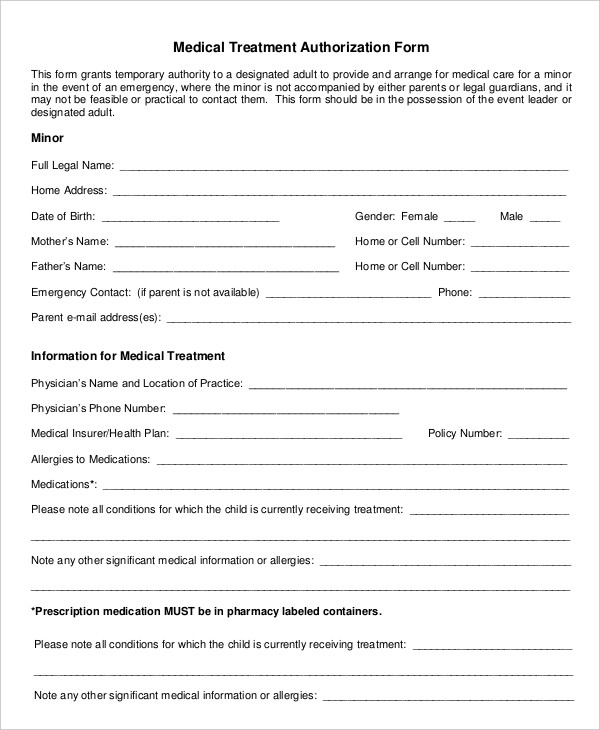
 Sample Medical Authorization Form Medical Forms Medical Consent Form Children Consent Forms Medical
Sample Medical Authorization Form Medical Forms Medical Consent Form Children Consent Forms Medical
 Medical Release Form For Minor Lovetoknow
Medical Release Form For Minor Lovetoknow
Comments
Post a Comment